





































 Ph.D. Equine Nutrition")

Andrew Peffers BVetMed Cert AVP (Equine Dentistry) BAEDT MRCVS Advanced Practitioner in Equine Dentistry
Below is a list of some of the clinical signs that a horse may exhibit if it has a dental problem:
1. Head tilt
2. Head tossing or head shaking
3. Bit chewing
4. Fighting the bit or going badly on one rein
5. Dropping food also known as quidding (Figure 1)
6. Weight loss
7. Drooling, foul breath
8. Smelly mucopurulent nasal discharge from one nostril
9. Facial swelling
10. Poor performance
If a horse is exhibiting any of these signs then it would at the very least require a detailed dental examination straight away. However, the aim with modern dentistry is to prevent health problems before they occur. Therefore, the minimum requirement for each horse is a dental check-up and rasping at least once every 12 months.
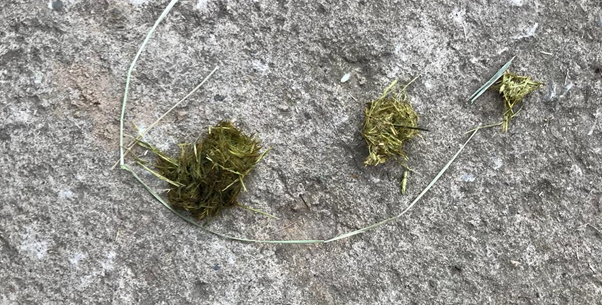
Figure 1. Balls of partially chewed hay on the floor of a stable from a horse that is quidding this is a classical sign of a horse with a dental problem.
WHY DO HORSE'S TEETH NEED RASPING?
Horses’ teeth are different to human teeth as they are hypsodont, meaning they keep erupting throughout the horse’s life. They erupt by approximately 2mm every year to replace the tooth that is worn down. The horse’s jaw is also anisognathic which means the upper jaw is wider than the lower jaw. Therefore, sharp edges form on the outside (buccal) edges of the upper teeth and on the inside (lingual) edges of the lower teeth. Unfortunately, because horses’ teeth are confined in a long narrow mouth it is very difficult for horse owners to examine their own horse’s teeth. For this reason, the majority of equine dental problems go unnoticed by horse owners. Post-mortem studies of horses’ heads show dental disease is present in over 50% of horses. Whereas the perceived incidence of dental disease as reported by owners is much lower. The conclusion to be drawn from these studies is that dental disease in horses is being underdiagnosed and this is why it is important that every horse has their teeth thoroughly examined at least once a year.
INCREASED EFFICIENCY OF EATING
A study by Johnson et al. (2017) was conducted to measure faecal fibre length pre- and post-dentistry and found there to be a significant decrease in mean faecal fibre length post-dentistry, suggesting increased efficiency of mastication and digestion of fibrous matter. Therefore, it could be concluded that regular dentistry improves eating efficiency. This study also revealed increased faecal fibre lengths in individuals with more severe dental abnormalities. In addition, studies have demonstrated a link between poor dental care and an increased incidence of both choke and colic (Hillyer et al., 2002; Cox et al., 2009). Again, highlighting the importance of regular dental care.
DENTAL DISEASES AFFECTING HORSES
EQUINE ODONTOCLASTIC TOOTH RESORPTION AND HYPERCEMENTOSIS (EOTRH)
This is a disease that primarily affects incisors but can also affect canines. It affects mostly older horses, generally 15 years or above, and its prevalence increases with the age of the horse. With this disease the incisors are painful and can become loose and even fracture. If a horse is reluctant to bite a carrot with their incisors this is often an early indicator that the horse has EOTRH. In addition, horses with EOTRH often resent having the dental gag put on for examination of the mouth. Horses with EOTRH show signs of gum inflammation, oedema and recession (Figure 2).

Figure 2. A horse with Equine Odontoclastic Tooth Resorption and Hypercementosis (EOTRH).
Excess calculus (dental plaque) may be laid down on the incisor where the gum has receded. There may also be obvious swelling of the gum caused by excessive cement laid down around the incisor root. In more advanced cases draining tracts may be obvious and the incisors become loose. Diagnosis is by taking x-rays of the incisors. Many different treatments have been tried to treat EOTRH including antibiotics, Chlorhexidine antiseptic cream (Dentisept®), steroids, surgical debridement of the inflamed gums, intra-oral splinting and even leaches. However, in the long-term these treatments are generally unsuccessful, and the best long-term treatment is to extract any incisors that are loose or painful. Owners fear that the horse will struggle to eat if they have their incisors extracted, however the opposite is normally true, and even horses that have had all their incisors extracted tend to eat better afterwards.
HOOKS
In some horses the upper and lower jaws do not align exactly. The usual presentation is that the upper jaw is slightly further forward than the lower jaw. Therefore, the teeth don’t wear down evenly, causing hooks to form on the front (rostral) edge of the first upper cheek teeth (106 and 206) and the back (caudal) edge of the last lower cheek teeth (311 and 411) (Figures 3 & 4).

Figure 3. A graphic depicting how rostral hooks and caudal ramps can form when the upper and lower jaws do not align perfectly.

Figure 4. A large upper rostral hook, this was so large it was causing soft tissue trauma on the opposite lower jaw, preventing the horse from eating.
Left untreated these hooks can grow so long that they start to dig into the soft tissues of the opposite jaw and will stop the horse being able to eat (Figure 5). As long as these teeth are rasped every 12 months this will stop these hooks from forming.

Figure 5. Tongue laceration caused by sharp rostral hook shown in figure 4.
STEP MOUTH
This is the term given when a whole tooth becomes dominant and is higher than the rest of the teeth in that arcade. This usually happens when a horse has lost a cheek tooth or had a cheek tooth removed. The opposing tooth has no tooth to wear against and therefore as the crown erupts by about 2-3mm a year, the tooth gets taller by 2-3mm a year. Another occasion when a step mouth occurs is when one adult tooth erupts earlier than its opposite tooth. These horses require dental visits twice a year to reduce the overgrowth.
WAVE MOUTH
A wave mouth can be thought of as an extension of a step mouth. A step mouth occurs when only one tooth in an arcade is dominant; a wave mouth occurs when two or three cheek teeth in an arcade are dominant (Figure 6).
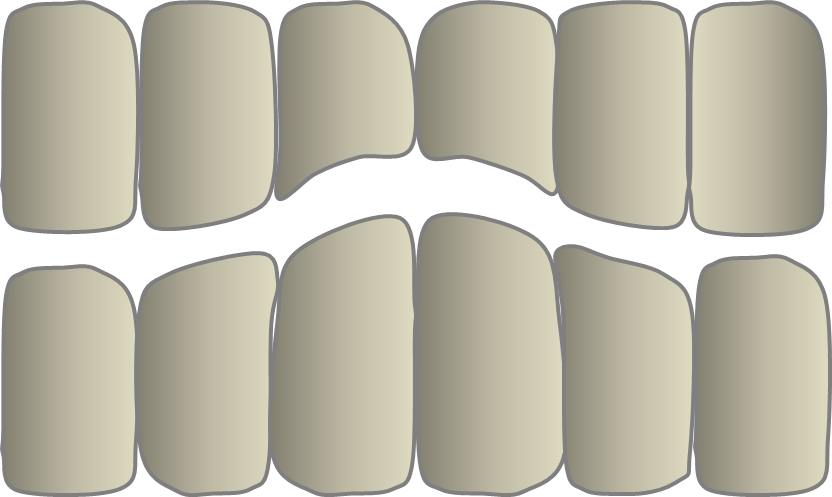
Figure 6. A graphic depicting a wave mouth.
The dominant teeth cause excessive wear on the opposing teeth on the opposite arcade. Thus, through excessive wear the opposing teeth become even more reduced. The dominant teeth then have less to wear against and erupt further, becoming even more dominant. So the cycle continues with the wave mouth gradually becoming worse each year. In most horses with a wave mouth the upper and lower arcade both have some dominant teeth, and some teeth showing excessive wear. The most common pattern is that the upper 06’s, 07’s, 10’s and 11’s are dominant and the upper 08’s, 09’s show excessive wear. The opposite pattern occurs on the lower teeth. Wave mouths are easily corrected if detected early. Horses with early wave mouths should have regular dental checks every 6 months and about 2-3mm should be removed from the dominant teeth each time. Normally within about two to three years of this treatment the cheek teeth arcades start to look normal.
SHEAR MOUTH
The occlusal (grinding) surface of normal molars is not flat but slopes downwards at an angle of approximately 15 degrees from the lingual (tongue) side to the buccal (cheek) side. In a shear mouth this angle can be greater than 45 degrees (Figure 7).

Figure 7. An example of shear mouth. The arcades on the left of the photograph are shear with table occlusal angles in excess of 45 degrees, the arcades on the right have a normal table angle.
DIASTEMA
A diastema is a gap between two teeth that is not normally present. Diastemata occur more frequently in the lower jaw than the upper jaw. The most common type of diastema is valve diastema; the teeth at the occlusal (chewing surface) are still quite closely opposed, while at the gingival (gum) margin the teeth are narrower forming a gap. Thus, these diastemata, when viewed from the side, are triangular in shape. Food debris is forced through the narrow gap at the top by the huge forces of chewing. This food packs into the bottom of the diastema, but because of the narrow opening at the top it cannot escape and is trapped (Figure 8).

Figure 8. An example of diastemata with food packing.
This trapped food then undergoes bacterial fermentation, releasing acid which damages the gum margin further. Therefore, the gum margins recede, which makes the diastema deeper and it becomes a self-perpetuating cycle. All diastemata once diagnosed should be treated. Basic treatment involves cleaning and flushing out diastema with picks, forceps and water irrigation. The gum margins are then treated with Chlorhexidine antiseptic cream (Dentisept®). In more advanced cases or in cases where the initial basic treatment has not worked, the diastema after cleaning can be filled with soft rubbery dental impression putty. Another treatment is to use a diastema burr to scallop a groove on the occlusal surface of the diastema to ease the pressure on the surface of the diastema and to prevent food being forced into the gap. The diet of the horse should be altered if possible to avoid haylage and sugary cereal based feeds as both of these have been implicated in the development of diastemata. It is also advisable to avoid short-chopped forage such as Alpha-A and chaff as these short chopped hard fibres can get stuck in the diastemata, and are uncomfortable for the horses and difficult to get out.
INFUNDIBULAR CARIES
Caries are holes or cavities in the hard tissues of teeth, for example the cement, dentine or enamel. One of the most common sites for caries in the horse is the infundibulum (Figure 9).

Figure 9. A grade 3 infundibular caries.
Only maxillary (upper) cheek teeth have infundibulae. The infundibulum is normally filled with cement. Studies of the infundibulae of maxillary cheek teeth have shown that many are incompletely filled with cement. This is known as cemental hypoplasia and is believed to be a factor in infundibular caries. Another factor is, as in humans, eating foods high in sugar that cause decay of the cementum. Deep infundibular caries can weaken the tooth and actually cause the tooth to fracture (Figure 10). Therefore it is highly recommended to fill infundibular caries if they are grade 2 or above.
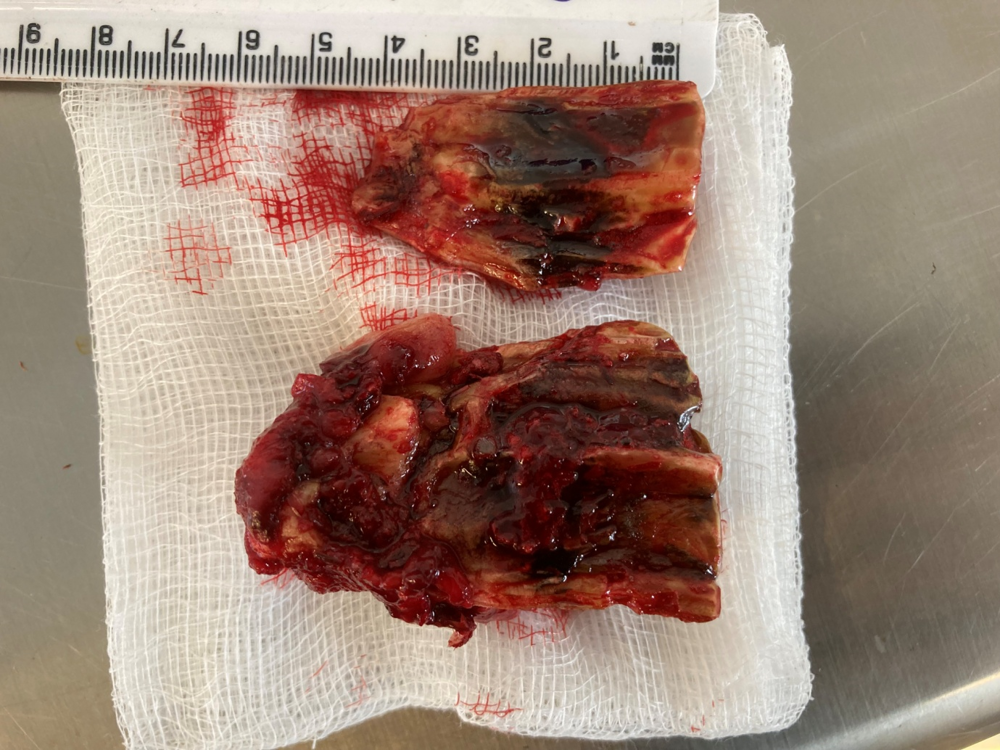
Figure 10. A tooth that has been extracted as it had fractured down the middle as a result of infundibular caries.
Hopefully this article has highlighted some of the dental conditions that horses suffer from, and the importance of regular dental examinations and rasping for all horses.
REFERENCES
Cox, R., Burden, F., Gosden, L., Proudman, C., Trawford, A., & Pinchbeck, G. (2009). Case control study to investigate risk factors for impaction colic in donkeys in the UK. Preventative Veterinary Medicine, 92(3): 179-187.
Hillyer, M.H., Taylor, F.G., Proudman, C.J., Edwards, G.B., Smith, J.E., & French, N.P. (2002). Case control study to identify risk factors for simple colonic obstruction and distension colic in horses. Equine Veterinary Journal, 34: 455-463
Johnson, C., Williams, J., & Philips, C. (2017). Effect of Routine Dentistry on Fecal Length in Donkeys. Journal of Equine Veterinary Science, 57: 41-45.