





































 Ph.D. Equine Nutrition")

Abigail Malone, BSc
WHAT IS COLIC AND WHAT ARE THE SIGNS?
Colic is the term used to describe a form of abdominal pain associated with a problem that occurs in the gastrointestinal tract (GT) of the horse (Frape, 2010). Unfortunately, colic is a common veterinary problem, accounting for one in three emergency vet call outs (Bowden et al., 2017). Horses who have previously had colic that has been treated either medically and/or surgically, are at risk of having recurring colic episodes (Gonçalves et al., 2002), evidenced by the finding that 11-16% of horses affected by colic have reoccurring colic episodes within a year (Scantlebury et al., 2011). Broodmares (Kaneene, 1997), Arabs (Cohen, 1999) and geldings (compared to stallions and mares) (Abutarbush et al., 2005) are thought to be at greater risk of colic although factors such as how the horse is managed and the diet it is fed are known to greatly influence the incidence of colic, meaning any horse of any age, breed or sex can be affected.
As colic does not discriminate, all horse, pony and donkey owners should be able to recognise colic symptoms and be aware of factors that increase the risk of colic. The symptoms of colic range from mild to severe (Table 1), with the worst cases resulting in death of the horse. Colic that initially looks mild can quickly escalate to a severe case, making it essential to always treat colic as a potentially serious condition and seek veterinary advice.
Scantlebury et al. (2014) highlighted how horse owners that understand when veterinary interventions are needed and who are aware of colic symptoms can help improve the outcome of a colic bout. They also emphasised that owners who understand how to manage horses appropriately will help to reduce the risk of colic issues. In a study by Bowden et al. (2020), involving 1564 horse owners, 55% of participants either did not know or gave incorrect values for their horse’s normal heart rate and respiratory rate, although 67% of owners were able to give the correct value for their horse’s normal rectal temperature. When asked what they would assess if they suspected their horse may have colic, 76% said faecal output, 75% said gastrointestinal sounds, 65% stated respiratory rate and 54% said heart rate. Overall, many owners were undecided on when they would deem it necessary to call their vet, although 61% felt confident that they could recognise most types of colic.
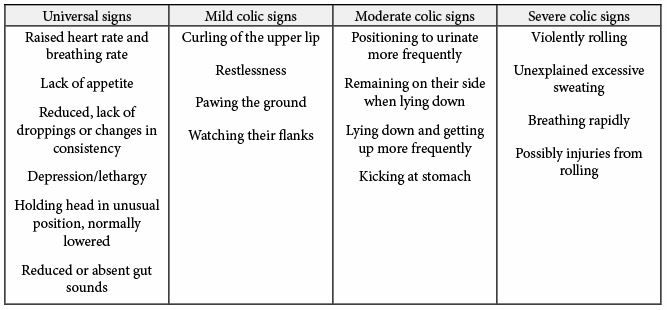
Table 1. Symptoms of colic in horses, ranging from mild to severe episodes.
This study also found that 54% of participants had experienced a horse dying from colic, showing that more horse owners need to be provided with the correct means to evaluate their horse’s normal clinical parameters and be able to recognise the early signs of colic to give their horse the best chance of survival and recovery.
TYPES OF COLIC AND THEIR RISK FACTORS
There are a number of different types of colic which can have either one or multiple causes and treatments. The cause of colic can be due to either nutritional factors, non-nutritional factors, or a combination of both, and for some cases of colic it may be difficult to pinpoint the original cause.
SPASMODIC COLIC
Spasmodic colic is the most commonly seen form of colic in horses (Greet & Rossdale, 1994), with one study by Proudman (1992) reporting that 72% of 200 colic cases were spasmodic. Spasmodic colic occurs when there are abnormal GT contractions due to an increase in bowel movements (Frape, 2010). These abnormal movements result in a cycle of painful spasms due to the GT being overactive, with spasms being either acute or lasting up to half an hour, and the cycle of spasms being over the period of a few hours. Spasmodic colic can occur at any point along the horse’s GT and cases are often mild. There are no specific nutritional risk factors associated with this form of colic, however high tapeworm infestation has been identified as a possible cause (Proudman et al., 1998).
IMPACTION COLIC
Another commonly seen form of colic is impaction colic. Impaction colic develops when the GT becomes blocked by a firm mass of ingesta (food that the horse has consumed and begun digesting), causing a build-up of fluid and gas which results in the GT becoming distended which is extremely painful (Frape, 2010). Impaction colic can occur in either the small intestine (SI) or the large intestine (LI), although it more frequently affects the LI. Impaction colic in the SI is likely to be found in the ilium or at the iliocaecal junction (the junction between the ileum and the caecum), whereas in the LI it can develop anywhere but normally at the pelvic flexure where the large colon narrows and bends back on itself (Greet & Rossdale, 1996; Towcester Equine Vets, 2021).
SAND COLIC
Sand colic is less common but can also cause a form of impaction. The impaction is due to the build-up of sand that has been ingested and then remains in the large colon of the LI (Frape, 2010). Sand cannot be expelled via the faeces as the heavy particles sink to the bottom of the colon, meaning that they do not pass along the GT with other normal ingesta particles which are expelled as faeces. Without treatment or removal of the sand, the particles begin to build up and cause irritation (Frape, 2010), with recurrent colic likely if the issue is not treated. Although sand colic may be less well known, for horse owners in sandy regions it is a real concern as their horses are more likely to ingest sand particles than horses living in non-sandy regions. Sand colic can be caused by horses in sandy regions grazing close to the ground due to low grass availability, or due to feeding horses from the ground in sand turnout pens or arenas (Walesby, 2004) (Figure 1). Signs of sand ingestion include weight loss, diarrhoea, and poor performance, so if you are concerned that your horse may have ingested sand, the recommendation is to seek veterinary and nutritional advice (Kendal et al., 2008).

Figure 1. Fields with limited grass cover increase the risk of horses consuming sand and dirt particles when eating. In areas with sandy soil this intake of sand may be excessive leading to sand irritation or colic.
GAS COLIC
As horses are hindgut fermenters, microbes aid digestion in the caecum and large intestine, where fibre is digested (Frape, 2010). Gas colic is often found in the LI due to excess gas being produced as a natural by-product of microbial fermentation in the LI, and occurs when the amount of gas being produced exceeds the amount of gas being removed (Frape, 2010). Gas colic cases can range from mild to very severe where it is possible for the LI to become distended and even twisted, causing excruciating pain. Gas colic is often found to be feed related which is discussed in the section on nutritional related risk factors.
DISPLACEMENTS, STRANGULATIONS & TORSIONS
These occur in the SI and LI and although they are less common, they can be incredibly serious cases. It must be noted that the mild signs of colic listed in Table 1 may be the early warnings that a more serious case of colic is about to develop, and therefore even mild signs must be monitored carefully. When a displacement occurs, a section of the horse’s intestines has moved to an abnormal area within the abdomen, for example right dorsal displacement is when the large colon moves to sit between the caecum and the right body wall causing obstruction and gas distention (University of Liverpool, 2021). This form of colic more often affects larger breeds or recently foaled mares (Towcester Equine Vets, 2021). Strangulations result in the blood supply to a section of the intestine becoming compromised. This type of colic is potentially the most serious and life-threatening (Towcester Equine Vets, 2021), although if detected early the horse has a greater chance of survival but will require emergency veterinary care and surgery. Unfortunately, it is common that the horse will need to be euthanised if strangulation occurs and is not treated quickly. Torsions are when the intestine twists on itself resulting in the blood supply being cut off to that area of the intestine. Broodmares in late pregnancy and post-foaling have been found to be particularly prone to this form of colic, which can develop rapidly causing fast deterioration of the horse in question, and death can occur anywhere from 4 to 24 hours from the onset of first symptoms (Rossdales Veterinary Surgeons, 2016).
FACTORS THAT MAY INCREASE THE RISK OF COLIC OCCURING
NUTRITIONAL FACTORS
A balanced and appropriate diet is key to a healthy horse, and unfortunately there are many nutritional factors from the stable to the field that can increase the risk of colic. As a horse owner it is important to choose good quality feed and forage to suit your horse’s nutritional needs.
Gas and impaction colic are almost always attributed to nutritional factors (Southwood, 2013). Dehydration can be a common cause of impaction colic due to the combination of reduced water intake and dry forage, therefore clean fresh water should always be made available.
Changes to the horse’s diet, either in the amount of each feedstuff fed, or the types of feed fed, should be made slowly to allow your horse’s microbial population to adapt to the nutrients that must be processed, and reduce the risk of colic (Garber et al., 2020) (see Your horse’s gut: gastrointestinal structure and function in JEN issue 1). Such gradual changes apply to all foodstuffs, including pasture and forage, and not just concentrate feeds. Other management changes should also be made slowly, including gradually changing your horse from different pastures. This is particularly important if the new pasture has ample grass coverage which horses may rapidly ingest. Restricting the amount of grass consumed will reduce overeating and let your horse adapt to the new grazing. Spring and autumn grass can contain considerable amounts of readily digestible carbohydrates and therefore can increase the risk of spasmodic colic, especially for horses who have had their grass intake limited or who have not been previously out at pasture (Purcell, 2005). Managing grass intake does not necessarily mean keeping horses stabled, as increasing pasture time can help to reduce the risk of recurring colic (Scantlebury et al., 2015) as it allows natural trickle feeding and promotes movement of ingesta along the GT.
A high concentrate diet, particularly if it is high in starch and in the form of a pellet, can increase the risk of impaction and gas colic. Large amounts of carbohydrate cannot be digested within the SI and so may reach the LI, causing the pH to drop which disrupts the balance of the microflora (Purcell, 2005). Recommendations are for horses to eat no more than 1g of starch per kg of bodyweight (Frape 2010), meaning fibre should form the majority of the horse’s diet (Pagan, 2007). This fibre is gained from grass and preserved forages, most commonly hay and haylage. Straw can also be fed as a low-calorie fibre source, although consuming too much straw is associated with increased risk of impaction colic due to the straw being of low digestibility, meaning it takes longer to break down within the GT (Harris et al., 2017). Straw should be introduced to the diet slowly and can comprise up to 30% of the forage portion, although it is not recommended for horses prone to colic and may not be suitable for all horses. Use of straw bedding should also be avoided for such horses due to the risk of them eating the bedding.
Sand and soil consumption is found more in horses who are fed forage from the floor, especially in arenas or sand paddocks, or in areas of sandy soil. To reduce the risk of sand consumption and sand colic, aim to keep horses' feed and forage off the ground by using haynets, or feeders with a solid bottom. Hay feeders have the benefit of letting horses eat with their head in a more natural, low position which promotes natural drainage of the respiratory system and promotes stretching of their back muscles.
NON-NUTRITIONAL FACTORS
As previously highlighted, management changes should also be made gradually where possible, as changes can cause horses to become stressed which may be linked to increased incidence of colic (Purcell, 2005).

Figure 2. Horses with stereotypic behaviours, particularly crib biting, are thought to increase the risk of colic episodes.
Stress may also be caused by high workloads which in turn can lead to exhaustion from overworking, and thus dehydration and lack of appetite which all contribute to the risk of colic (Frape, 2010). Stress may result in stereotypic behaviours, such as crib biting and windsucking, which have been found to increase the risk of colic episodes although further research is needed to determine the type and severity of colic associated with such behaviours (Malamed et al., 2010) (Figure 2). Scantlebury et al. (2014) and Archer et al. (2008) also report that crib biting and windsucking increase the risk of colic alongside weaving. Stress may also be caused by box rest or reduced turnout or exercise, which has already been highlighted to increase the risk of colic due to reduced movement of ingesta along the GT (Towcester Equine Vets, 2021). Increased time in the stable may also reduce the overall amount of fluid consumed, as horses eat greater amounts of preserved forages which contain less moisture compared to grass. Such changes are particularly evident in autumn and winter when horses may be stabled more due to weather variations. Diakakis & Tyrnenopoulou (2017) found a positive correlation between sudden temperature changes and the incidence of colic, particularly between the colder and warmer seasons.
Maintaining good management practices and a parasite control programme are also essential to reducing the risk of colic. Keeping stables and fields clean and removing faeces should form a key part of parasite control programmes, as should testing for parasite burdens to identify animals requiring anthelmintic treatment (Frape, 2010). Dental care should also be part of your horse’s routine management and should not be overlooked as a potential contributing factor to the cause of colic. Maintaining a dental care routine will ensure that food can be chewed properly which reduces particle size and promotes breakdown of ingesta (Purcell, 2005). Chewing also stimulates saliva production which helps to buffer the acidic stomach of the horse and maintain a healthy GT.
SUMMARY
Our knowledge of colic and its risk factors has developed greatly over recent years to allow us to better understand, prevent and treat colic. Despite these advances, it may still be difficult for some owners to recognise the symptoms of colic, and the severity of the colic episode. As such, knowing when to seek veterinary advice can be challenging, which is why it is recommended for owners to contact the vet as soon as colic is suspected, even for what seems like a mild case, as it can quickly deteriorate into a more severe issue requiring emergency veterinary intervention. Each case should be assessed individually and whilst there are many possible nutritional and non-nutritional factors, owners should consider all possible risks to reduce the occurrence of colic. Aim to keep the horse’s diet as natural as possible by feeding approximately 2% of their body weight per day with the majority of their diet comprising of forage. Avoid overfeeding high carbohydrate feed and allow regular turnout. Finally, feeds should be offered in small amounts and at regular intervals to mimic the natural trickle feeding behaviour of equids.
REFERENCES
Abutarbush, S.M., Carmalt, J.L., & Shoemaker, R.W. (2005). Causes of gastrointestinal colic in horses in western Canada: 604 cases (1992 to 2002). Canadian Veterinary Journal, 46(9): 800-805.
Archer, D.C., Pinchbeck, G.L., French, N.P., & Proudman, C.J. (2008). Risk factors for epiploic foramen entrapment colic: An international study. Equine Veterinary Journal, 40(3): 224-230.
Bowden, A., Burford, J.H., Brennan, M.L., England, G.C.W., & Freeman, S.L. (2020). Horse owners’ knowledge, and opinions on recognising colic in the horse. Equine Veterinary Journal, 52 (2) 262-267.
Bowden, A., England, G.C.W., Burford, J.H., Mair, T.S., Furness, W., & Freeman, S.L. (2017). Prevalence and outcome of conditions seen at out-of-hours primary assessment at two practices over a 3-year period (2011-2013). Equine Veterinary Journal, 49(51): 5-29.
Cohen, N., Gibbs P., & Woods, A. (1999). Dietary and other management factors associated with equine colic. Proceedings of the Annual Convention of the AAEP, 45:96-98.
Diakakis, N., & Tyrnenopoulou, P. (2017). Correlation between equine colic and weather changes. Journal of the Hellenic Veterinary Medical Society, 68(3): 455-466.
Frape, D. (2010). Equine Nutrition and Feeding, 4th Ed. Wiley-Blackwell, Oxford, UK.
Garber, A., Hastie, P., & Murray, J.-A. (2020). Factors influencing equine gut microbiota: current knowledge. Journal of Equine Veterinary Science, 88: 102943.
Gonçalves, S., Julliand, V., & Leblond, A. (2002). Risk factors associated with colic in horses. Veterinary Research, 33: 641-652.
Greet, T.R.C., & Rossdale, P.D. (1996). The Digestive System. In: Rossdale, P.D. (eds.) Veterinary Notes for Horse Owners. Stanley Paul, London, UK.
Harris, P.A., Ellis, A.D., Fradinho, M.J., Jansson, A., Julliand, V., Luthersson, N., Santos, A.S., & Vervuert, I. (2017). Review: Feeding conserved forage to horses: recent advances and recommendations. Animal, 11(6): 958-967.
Kaneene, J.B., Miller, R., Ross, W.A., Gallagher, K., Marteniuk, J., & Rook, J. (1997). Risk factors for colic in the Michigan (USA) equine population. Preventative Veterinary Medicine, 30(1): 23-26.
Kendal, A., Ley, C., Egenvall, A., & Brojer, J. (2008). Radiographic parameters for diagnosing sand colic in horses. Acta Veterinaria Scandinavia, 50(17).
Malamed, R., Berger, J., Bain, M.J., Kass, P., & Spier, S.J. (2010). Retrospective evaluation of crib-biting and windsucking behaviours and owner-perceived behavioural traits as risk factors for colic in horses. Equine Veterinary Journal, 42 (8): 686-692.
Mcgovern, K.F., Baldon, B.M., Fraser, B.S.L., Boston, R.C. (2012) Attempted Medical Management of Suspected Ascending Colon Displacement in Horses. Veterinary Surgery. 41 (3): 399-403
Pagan, J.D. (2007). Causes, risks of colic explained. Feedstuffs, 79(7).
Proudman, C.J. (1992). A two year, prospective survey of equine colic in general practice. Equine Veterinary Journal, 24(2): 90-93.
Proudman, C.J., French, N.P., & Trees, A.J. (1998). Tapeworm infection is a significant risk factor for spasmodic colic and ileal impaction colic in the horse. Equine Veterinary Journal, 30(3): 194-199.
Purcell, K. (2005). An ounce of prevention: Feeding management to minimize colic. Advances in Equine Nutrition Volume 3: 121- 126.
Rossdales Veterinary Surgeons (2016). Published on the Internet; https://www.rossdales.com/assets/files/Colic-and-colon-torsion-in-the-mare.pdf. [Accessed 26 July 2021]
Scantlebury, C.E., Archer, D.C., Proudman C.J., & Pinchbeck, G.L. (2011). Recurrent colic in the horse: Incidence and risk factors for recurrence in the general practice population. Equine Veterinary Journal, 43(39): 81-88.
Scantlebury, C.E., Archer, D.C., Proudman C.J., & Pinchbeck, G.L. (2015). Management and horse-level risk factors for recurrent colic in the UK general equine practice population. Equine Veterinary Journal, 47(2): 202-206.
Scantlebury, C.E., Perkins, E., Pinchbeck, G.L., Archer D.C., & Christley, R.M. (2014). Could it be colic? Horse-owner decision making and practices in response to equine colic. BMC Veterinary Research, 10 (S1).
Southwood, L.L. (2013). Practical Guide to Equine colic. Wiley-Blackwell, Chichester, UK.
Towcester Equine Vets (2021). Colic. Published on the Internet; https://towcester-vets.co.uk/equine/services/colic/. [Accessed 25 July 2021]
University of Liverpool (2021). Colic types and causes. Published on the internet; https://www.liverpool.ac.uk/media/livacuk/equine/documents/colic-types-and-causes.pdf. [Accessed 25 July 2021]
Walesby, H.A., Blackmer, J.M., & Berthelot, A. (2004). Equine Sand Colic. Compendium on continuing education for the practicing veterinarian, 26(9): 712-719.